Understanding Biofilm Risks in Hospital Sinks: A Proactive Water Management Guide
We understand that preventing infections is a top priority in healthcare facilities, and sometimes, the biggest threats are hiding in plain sight. Today, we’re diving into a critical area of concern: the humble hospital sink. These seemingly innocuous fixtures can become breeding grounds for dangerous biofilms and resistant bacteria, posing a serious risk to patient safety. While tap water in the United States meets stringent safety standards, it is not sterile, and certain conditions within hospital plumbing can foster microbial growth to dangerous levels.
Join us as we explore how these risks emerge, what measures we can take, and how a proactive water management guide can safeguard our patients from pathogens lurking within hospital sinks.
The Unseen Threat: Understanding Biofilms and Pathogen Transmission from Hospital Sinks
Believe it or not, a hidden city of potentially harmful microbes may be thriving in hospital drains. These microbial cities, known as biofilms, are complex communities of bacteria encased in a protective slimy layer. Despite robust infection prevention protocols, these biofilms are increasingly linked to healthcare-associated infections (HAIs). The drains in healthcare settings are frequently found to be contaminated with a variety of microorganisms, including Gram-negative and antibiotic-resistant bacteria. This poses a silent but significant threat that demands closer inspection and a strategic defense.
How Dangerous Biofilms Form and Thrive in Hospital Sinks and Drains
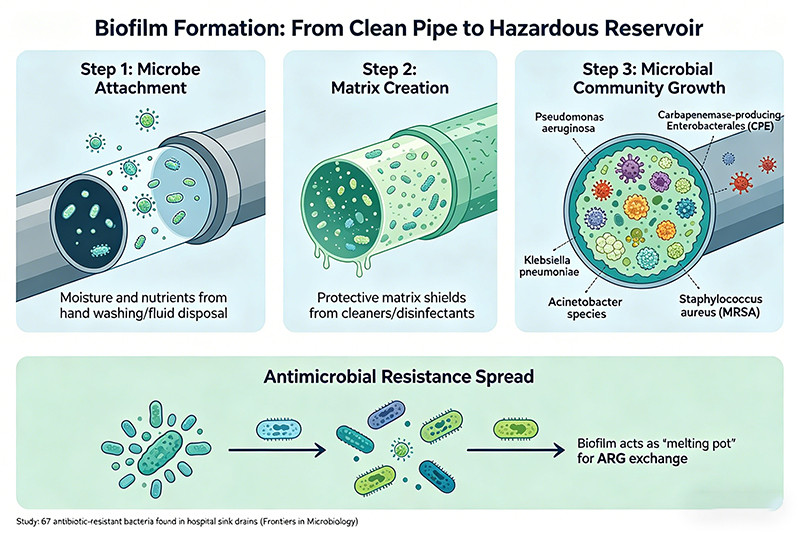
The formation of a biofilm is a systematic process that turns a clean pipe into a hazardous reservoir. It begins when free-floating microbes attach to the inner surfaces of drainpipes—a process facilitated by the constant moisture and available nutrients. Everyday activities, such as hand washing and the disposal of fluids, supply the very bacteria and nutrients that fuel the growth of these biofilms.
Once attached, these microorganisms create a sticky, protective matrix of proteins and polymers, shielding them from cleaning agents and disinfectants. This protective layer is a key reason why traditional cleaning methods often fail; while they may kill free-floating microbes, they can't penetrate the biofilm's core, allowing it to regrow rapidly. Inside this shelter, a diverse community of bacteria, including molds, yeasts, and viruses, can flourish.
This environment is particularly dangerous because it acts as a "melting pot" for antimicrobial resistance. Bacteria within the biofilm can exchange genetic material, allowing antibiotic resistance to spread between different species. Studies have found that hospital sink drains are key reservoirs for opportunistic pathogens and antimicrobial resistance genes (ARGs). Common pathogens found thriving in these biofilms include:
- Pseudomonas aeruginosa: A leading cause of ventilator-associated pneumonia and sepsis.
- Carbapenemase-producing Enterobacterales (CPE): A family of bacteria highly resistant to last-resort antibiotics.
- Klebsiella pneumoniae: A common cause of HAIs.
- Acinetobacter species: Notorious for their resilience in hospital environments.
- Staphylococcus aureus: Including methicillin-resistant strains (MRSA).
A study published in Frontiers in Microbiology identified 67 different types of bacteria in hospital sink drains, many of which were resistant to multiple antibiotics. This underscores the critical challenge that even rigorous cleaning protocols face, as routine disinfection often fails to eradicate these entrenched microbial communities.
The Silent Spread: How Pathogens from Hospital Sinks Reach Vulnerable Patients
The journey of a pathogen from the drain to a patient is often invisible and dangerously efficient. It's a common misconception that since patients don't touch the inside of drains, the risk is minimal. However, research has clearly shown multiple pathways for transmission. The primary mechanism is splashing.
When water from a faucet hits the drain, it can aerosolize and splash droplets containing bacteria onto the surrounding environment. This area, known as the "splash zone," can extend up to three feet from the sink. One study demonstrated that running water over a contaminated sink strainer could disperse E. coli up to 30 inches away.
These contaminated droplets can land on:
- Healthcare workers' hands and clothing: From where they can be transferred to patients during care activities.
- Patient care items: Such as medication trays, sterile supplies, and medical equipment left near the sink.
- The patient's personal items: Including toothbrushes or water cups.
- The patient directly: Especially if their bed is located close to the sink.
Studies have directly linked pathogens found in sinks to patient infections through genomic sequencing. A study in Israel found that of 318 patients who acquired CPE, 40% had a contaminated sink with the same strain identified in their room where no other source was detected. In some cases, the contamination was present in the sink before the patient was even admitted, proving the sink was the likely source.
Surprisingly, handwashing, the very activity sinks are designed for, accounts for a small fraction of their use in healthcare settings. They are more frequently used for other tasks like medical care, nutrition, and environmental cleaning, all of which present opportunities for contamination. The table below illustrates the various pathways through which pathogens can spread from a sink.
| Transmission Pathway | Description | High-Risk Scenarios |
|---|---|---|
| Direct Splash | Water droplets carrying pathogens are ejected from the sink basin during use. | High-pressure faucets, shallow sink bowls, faucet stream aimed directly at the drain. |
| Aerosolization | Microscopic droplets become airborne and can be inhaled or settle on distant surfaces. | Flushing toilets, high-pressure water streams. |
| Fomite Contamination | Items placed within the splash zone become contaminated. | Storing medical supplies, preparing medications, or placing personal items on countertops near sinks. |
| Healthcare Worker Vector | Staff members' hands or uniforms are contaminated by touching the sink or by splashes. | Washing hands in a contaminated sink, then proceeding to patient care without proper drying or re-sanitizing. |
These pathways highlight that the sink is not an isolated fixture but an active hub within the patient care environment, capable of silently dispersing dangerous, drug-resistant organisms.
Our Proactive Measures: Innovative Solutions for Safer Hospital Sinks
Recognizing the sink as a critical control point for infection prevention requires a shift from reactive cleaning to proactive management. This involves a two-pronged approach: re-evaluating the physical interventions we use to control contamination and redesigning the human behaviors that interact with these fixtures. By pairing innovative technology with smarter practices, healthcare facilities can create a more resilient defense against waterborne pathogens.
Evaluating Past and Present Interventions for Contaminated Hospital Sinks
Historically, the response to sink contamination has centered on periodic cleaning and disinfection. Traditional methods have included:
- Manual Cleaning: Regular scrubbing of sink basins and faucets with hospital-grade disinfectants.
- Chemical Disinfection: Pouring disinfectants like chlorine or hydrogen peroxide down drains to kill microbes.
- Hot Water/Steam Flushing: Using thermal energy to disinfect pipes and drains.
However, these interventions have significant limitations. While they may offer a temporary reduction in microbial load, they often fail to eliminate the underlying biofilm. Studies have shown that even after chemical disinfection, bacterial populations can rebound to their original levels within days, or sometimes even hours. Chlorine-based disinfectants, for instance, have proven ineffective in reducing bacterial concentration within established biofilms. Even more concerning is that some disinfectants, when used at low concentrations, may inadvertently promote the exchange of antibiotic resistance genes among bacteria.
More recent innovations have aimed to improve the efficacy of disinfection. Foam-based disinfectants, for example, are designed to increase contact time within the drain, allowing for better penetration into the biofilm. A study comparing various foam products found that a formulation of hydrogen peroxide and peracetic acid was most effective, suppressing gram-negative bacteria for at least three days. However, even these advanced methods often require frequent, repeated application to prevent regrowth, highlighting that disinfection alone is a short-term solution. The persistent nature of biofilms demands a more integrated strategy that goes beyond periodic chemical attacks.
Embracing Advanced Design and Behavioral Strategies for Enhanced Safety in Hospital Sinks
A truly proactive approach marries smarter technology with educated human behavior. The goal is to create an environment where contamination is less likely to occur in the first place and where staff are equipped with the knowledge to minimize risks.
Key behavioral strategies, often guided by CDC recommendations, include:
- Defining the "Splash Zone": Strictly enforcing a designated area of approximately three feet around the sink where no patient care items, medications, or personal belongings are placed.
- Proper Waste Disposal: Prohibiting the disposal of bodily fluids, IV solutions, and liquid nutrition down patient-room sinks, as these provide rich nutrients for biofilm growth.
- Hand Hygiene Discipline: Educating staff on the nuances of sink use. One observational study found that sinks were used for waste disposal 60% of the time, while handwashing occurred only 10% of the time. Staff should use alcohol-based hand sanitizer after touching sink fixtures and understand which sinks are designated for hand hygiene versus waste disposal.
These behavioral modifications are most effective when supported by superior environmental design.
Exploring how innovative hospital sinks, like those from Samsink, offer improved design features to mitigate splash and enhance hygiene, contributing to overall safety.
The physical design of a sink plays a monumental role in infection control. Many traditional hospital sinks have features that inadvertently promote contamination, such as shallow bowls that increase splashing, faucets positioned directly over the drain, and materials that are difficult to clean. Recognizing these flaws, manufacturers are developing a new generation of sinks with safety engineered into their very structure.
Innovative sinks, such as those developed by companies like Samsink, incorporate multiple features designed to minimize the risks associated with biofilms and splash:
1. Splash Reduction:
- Deep, Sloped Basins: A deeper bowl contains water more effectively, while sloped surfaces encourage water to drain away rather than pool. This design physically limits the distance that droplets can travel.
- Offset Faucets: Positioning the faucet so that the water stream hits the side of the basin instead of the drain directly is a simple but highly effective way to reduce the aerosolization of microbes from the P-trap.
- Advanced Fin Technology: Some modern sinks feature an innovative fin molded into the basin, which is engineered to deflect the water stream and has been shown to reduce splashing by over 90%.
2. Enhanced Drainage and Hygiene:
- Smooth, Vertical Drains: Designs that ensure water drains quickly and vertically through smooth pipes, free of hanging points or steps, prevent water from pooling and becoming stagnant—a key contributor to biofilm growth.
- Antimicrobial Surfaces: The use of materials with antimicrobial properties, such as copper components or specially treated glazes, can make it more difficult for bacteria to adhere to surfaces and begin forming a biofilm.
3. Ease of Maintenance:
- Touch-Free Operation: Sensor-operated or elbow-operated controls eliminate the need for hand contact, reducing cross-contamination between healthcare workers.
- Designed for Disassembly: Some modern taps and fixtures are designed to be easily detached and dismantled, allowing for thorough cleaning and disinfection of all components—a major step forward in eliminating hidden reservoirs of bacteria.
By investing in these advanced designs, healthcare facilities can fundamentally re-engineer one of the most critical points of vulnerability in the patient care environment, creating a foundation of safety that is less reliant on fallible human processes alone.

Building a Robust Defense: A Comprehensive Water Management Program for Hospital Sinks
A reactive approach of simply cleaning what is already contaminated is not enough. To truly safeguard patients from waterborne pathogens originating in sinks, healthcare facilities must build a systematic, proactive defense. This defense is anchored by a comprehensive water management program that treats the entire building's water system as an interconnected ecosystem, with sinks identified as critical control points.
The Imperative for a Dedicated Water Management Plan Addressing Hospital Sinks and Water Systems
A Water Management Program (WMP) is no longer just a best practice; it's a regulatory necessity. In June 2017, the Centers for Medicare & Medicaid Services (CMS) issued a directive requiring hospitals and other healthcare facilities to develop and implement WMPs that align with industry standards, specifically ASHRAE Standard 188. This mandate shifted the paradigm from voluntary action to a required condition for participation in Medicare and Medicaid programs.
The core purpose of a WMP is to minimize the risk of waterborne pathogen growth and spread, with a primary focus on Legionella, but also encompassing other opportunistic pathogens like Pseudomonas and nontuberculous mycobacteria that thrive in sink biofilms. A WMP is not a one-time task but a continuous cycle of assessment, management, and validation.
Key components of a WMP include:
- System Analysis: Creating detailed diagrams that map the flow of water throughout the facility, from its point of entry to every endpoint, including every single sink.
- Hazard Identification: Pinpointing areas where hazardous conditions—such as water stagnation, inadequate temperatures, or low disinfectant levels—could promote microbial growth. Sinks and their P-traps are universally considered high-risk areas.
- Control Measures: Establishing specific procedures to manage these risks. This includes defining acceptable ranges for water temperature and disinfectant levels and documenting corrective actions for when these limits are not met.
- Monitoring and Documentation: Implementing a rigorous schedule for monitoring control measures and meticulously documenting all results. This documentation is crucial for demonstrating compliance during surveys by organizations like The Joint Commission.
For sinks specifically, the WMP must address the unique risks they pose. This involves developing strategies for routine cleaning, managing the "splash zone," and creating policies for appropriate use, ensuring they are not used for the disposal of nutrient-rich waste that feeds biofilms.
Assembling Your Multidisciplinary Team for Effective Water Management and Controlling Hospital Sinks
An effective WMP cannot be managed in a silo. Its success hinges on the collaboration of a multidisciplinary team, where each member brings a unique expertise and perspective. The CDC and ASHRAE both emphasize the importance of this team-based approach.
A well-rounded Water Management Team typically includes:
| Role | Key Responsibilities in Sink and Water Management |
|---|---|
| Infection Preventionist (IP) | Serves as the clinical expert on pathogen transmission. The IP's role is to conduct risk assessments related to patient populations, identify high-risk areas (like ICUs or transplant units), connect clusters of infections to potential water sources, and educate staff on safe practices around sinks. |
| Facilities Engineer | The technical expert on the building's infrastructure. This individual is responsible for maintaining the plumbing systems, managing water temperatures and disinfectant levels, implementing and overseeing maintenance schedules, and understanding the physical layout of the pipes that connect the sinks. They are the "system owner." |
| Hospital Administrator/Leadership | Provides the necessary authority, resources, and budget to support the WMP. Leadership buy-in is critical for ensuring the program is prioritized and that corrective actions, such as replacing old sinks or plumbing, can be funded and implemented. |
| Environmental Services (EVS) Manager | Oversees the staff responsible for the daily cleaning and disinfection of hospital rooms, including the sinks. This person ensures that cleaning protocols are correctly implemented, staff are properly trained, and the right products are used for sink hygiene. |
| Clinical Lab Representative | Manages the collection and analysis of water samples for microbial testing. They provide the data that validates whether the WMP is working and can help identify specific pathogens during an outbreak investigation. |
| Clinicians/Nursing Staff | Act as the frontline observers. Nurses and doctors are the ones who use sinks most frequently and can provide invaluable feedback on sink design, functionality, and employee behavior. They are also crucial for championing safe practices on their units. |
This collaborative approach ensures that the WMP is not just a document but a living program integrated into the hospital's daily operations. The facilities engineer knows the pipes, the IP knows the pathogens, and the administrative leader ensures they have the tools to fight them. Together, they form a robust defense system to protect patients from the hidden dangers within the water system.
Upholding Standards: CDC Guidelines and Regulatory Compliance for Hospital Sinks Safety
Achieving lasting safety and control over pathogens in hospital sinks is not a one-off project but a continuous commitment to excellence. This commitment is guided by national standards and regulatory requirements, centrally driven by the Centers for Disease Control and Prevention (CDC). By translating these high-level guidelines into daily operational practices and integrating them into a long-term strategic vision, healthcare facilities can build a durable and effective defense.
Implementing Practical CDC Recommendations for Daily Operations and Maintenance of Hospital Sinks
The CDC provides clear, actionable guidance to minimize the risks associated with hospital sinks. These recommendations are designed to be integrated into routine cleaning protocols and staff behavior. Adherence to these practices is foundational to any successful water management program.
A practical checklist for daily operations, based on CDC guidelines, should include:
Behavioral and Usage Protocols:
- Prohibit Inappropriate Disposal: Staff must be trained to never pour bodily fluids, IV medications, or liquid nutritional supplements down patient room or handwashing sinks. These substances act as a food source for biofilms. Discard them in appropriate solid waste containers or designated utility sinks.
- Maintain the "Splash Zone": Keep a clear three-foot radius around the sink free of all patient care items, medications, and personal belongings. Use splash guards if medication prep areas are unavoidably close to a sink.
- Hand Hygiene Discipline: Use alcohol-based hand rub as the preferred method for hand hygiene unless hands are visibly soiled. After washing hands with soap and water, avoid touching faucet handles with clean hands.
Cleaning and Disinfection Protocols:
- Daily Surface Disinfection: At least once per day, clean and disinfect all high-touch surfaces around the sink. This includes the sink basin, faucet, handles, and surrounding countertops.
- Use EPA-Registered Disinfectants: Select products registered with the Environmental Protection Agency (EPA) that are effective against the pathogens likely to be found in a healthcare environment. Always follow the manufacturer's instructions for concentration, contact time, and safe use.
- Address Biofilms During Outbreaks: During a suspected or confirmed outbreak linked to a water source, the CDC advises considering the use of an EPA-registered disinfectant with specific claims for biofilm removal in drains.
Physical and Engineering Checks:
- Regularly Clean Aerators: Faucet aerators can trap sediment and become colonized with bacteria. They should be cleaned regularly as part of the maintenance schedule.
- Monitor Water Flow: Ensure water pressure is regulated to minimize splashing.
- Inspect for Stagnation: Routinely flush infrequently used outlets to prevent water from stagnating, which allows biofilms to grow.
Here is a sample operational chart for EVS staff:
| Task | Frequency | Procedure |
|---|---|---|
| Surface Cleaning | Daily | Wipe down sink basin, faucet, handles, and countertops with an approved hospital disinfectant. |
| Splash Zone Check | Every Shift | Ensure the 3-foot area around the sink is clear of supplies and personal items. |
| Drain Inspection | Daily | Visually inspect drains for blockages or visible biofilm and report to facilities. |
| P-Trap Flushing | Per WMP Schedule | Flush infrequently used sinks with hot water for the duration specified in the facility's Water Management Plan. |
The Path Forward: Achieving Long-Term Contamination Control in Hospital Sinks Through Integrated Strategies
Controlling sink contamination is a complex challenge that requires moving beyond isolated interventions. A long-term, sustainable strategy must integrate multiple lines of defense: engineering controls, administrative policies, and behavioral reinforcement. This "big picture" approach is the future of water safety in healthcare.
1. Integration of Design and Practice: The path forward lies in facilities making smarter choices from the ground up. During new construction or renovations, prioritize the installation of sinks with proven safety features—deep basins, offset faucets, splash-reducing designs, and hygienic materials. These engineering solutions create an inherently safer environment that makes good practices easier to follow. For existing facilities, retrofitting with safer faucets, installing splash guards, and reconfiguring paper towel and soap dispensers outside the splash zone are critical investments.
2. Emphasis on a Holistic Water Management Program: The established Water Management Program must be a dynamic, living entity. It should extend beyond Legionella control in cooling towers to address the entire premise plumbing system, with a special focus on sink drains and distal outlets. This requires a commitment to regular risk assessments, consistent monitoring, and honest program validation. A key part of this is data-driven decision-making. Regular water sampling can identify trends and provide early warnings, allowing the WMP team to act before an outbreak occurs.
3. Continuous Education and Competency: Policies and protocols are only effective if they are understood and followed. Long-term success depends on a sustained commitment to staff education and training. This training should not be a one-time event but a continuous process that includes competency assessments. Staff must understand the "why" behind the rules—how a simple act like pouring coffee down a sink can contribute to a patient's infection.
4. Embracing Innovation: The field of infection control is constantly evolving. Healthcare facilities must remain open to new technologies and methodologies. This could include automated disinfection systems that inject sanitizing agents into drain lines, advanced materials with superior antimicrobial properties, or "smart" sinks that monitor their own usage and cleanliness.
Ultimately, achieving long-term control is about creating a culture of safety where every member of the healthcare team—from the CEO to the EVS staff—recognizes the sink not as a simple fixture, but as a critical piece of medical equipment that demands the same level of respect and diligence as any other tool used in patient care. This integrated, multidisciplinary approach is the only way to effectively mitigate the persistent threat of sink-related infections.
Key Takeaways
To effectively manage the risks posed by hospital sinks, a multi-layered and proactive strategy is essential. Here are the key takeaways from our guide:
- Sinks are High-Risk Reservoirs: Hospital sinks, particularly the drains and P-traps, are ideal breeding grounds for dangerous biofilms that harbor antibiotic-resistant pathogens like Pseudomonas aeruginosa and Carbapenem-resistant Enterobacterales (CPE).
- Splashing is the Primary Threat: Pathogens spread from drains to patients primarily through splashing. This "splash zone" can contaminate healthcare workers' hands, patient care items, and the surrounding environment up to three feet away.
- Traditional Cleaning is Insufficient: Routine cleaning and pouring disinfectants down drains are often ineffective against established biofilms, which can regrow rapidly. A more robust and frequent intervention strategy is needed for long-term control.
- Design Matters: Proactive prevention starts with better sink design. Features like deep basins, offset faucets that don't flow directly into the drain, and splash-reducing technologies are crucial engineering controls that minimize contamination risk.
- A Water Management Program (WMP) is Mandatory: All healthcare facilities are required by CMS to have a comprehensive WMP aligned with ASHRAE 188. This plan must identify, manage, and monitor risks throughout the building's entire water system, with sinks being a critical focus.
- Collaboration is Crucial: Effective water management requires a multidisciplinary team, including Infection Prevention, Facilities Engineering, EVS, leadership, and clinical staff. Each role provides essential expertise for a holistic defense.
- Adherence to CDC Guidelines is Key: Daily operations must incorporate CDC recommendations, such as prohibiting the disposal of nutrient-rich fluids in sinks, maintaining a clear splash zone, and performing consistent, documented cleaning of all sink surfaces.
- Long-Term Control Requires an Integrated Approach: Lasting success depends on combining smart engineering (better sinks), robust administrative controls (a dynamic WMP), and consistent behavioral practices (staff education and adherence) to create a resilient culture of safety.
Frequently Asked Questions (FAQ)
Q1: What exactly is a biofilm and why is it so hard to remove from sink drains? A: A biofilm is a complex community of microorganisms, including bacteria, fungi, and viruses, that attach to a surface and encase themselves in a slimy, protective matrix. This matrix shields them from disinfectants and mechanical cleaning, making them incredibly resilient. In a sink drain, the constant moisture and supply of nutrients from disposed liquids create a perfect environment for biofilms to thrive, allowing them to become a persistent reservoir for pathogens.
Q2: How far can bacteria splash from a hospital sink? A: Studies have shown that bacteria can splash out of a sink and contaminate an area up to three feet away. This is known as the "splash zone." Droplets can land on countertops, medical equipment, healthcare workers' clothing, and even patients if they are too close to the sink.
Q3: Are chemical disinfectants effective at clearing biofilms from drains? A: While chemical disinfectants can kill some free-floating bacteria, they are often ineffective at completely eradicating established biofilms. The protective matrix of the biofilm prevents deep penetration, and bacterial colonies can regrow quickly, sometimes within just a few days. More advanced methods like foam disinfectants or thermal treatments may be more effective but often require repeated application as part of a structured maintenance plan.
Q4: What is the single most important design feature to look for in a safer hospital sink? A: While several features contribute to safety, one of the most critical is an offset faucet that directs the water stream away from the drain. When water hits the drain directly, it is highly likely to aerosolize and splash bacteria from the biofilm upwards and out of the sink. By having the water hit the side of the basin, this primary mechanism of transmission is significantly reduced.
Q5: Who is responsible for managing sink safety in a hospital? A: Sink safety is a shared responsibility managed by a multidisciplinary Water Management Team. Key players include:
- Facilities Engineering: For the physical maintenance of plumbing and water systems.
- Infection Prevention: For risk assessment, surveillance, and policy development.
- Environmental Services (EVS): For daily cleaning and disinfection protocols.
- Hospital Leadership: For providing resources and enforcing compliance.
- Clinical Staff: For adhering to safe usage practices daily.
Q6: Can we eliminate risks by simply removing sinks from patient rooms? A: While some studies have shown a reduction in infections after removing sinks from ICUs, this is an extreme measure that is not practical for most healthcare settings. Sinks are essential for hand hygiene, which remains a cornerstone of infection prevention. The more sustainable solution is to make sinks safer through better design, smarter usage protocols, and a comprehensive water management program rather than eliminating them entirely.
We've seen that the challenge of controlling pathogens in hospital sinks is complex, requiring a multi-faceted and continuous effort. These fixtures, essential for hand hygiene, can paradoxically become sources of infection if not managed with vigilance and scientific rigor.
By understanding the science behind biofilm formation and transmission, embracing both traditional and innovative interventions, and implementing robust water management plans, we can significantly reduce the risks associated with hospital sinks. It is the combination of smarter design, educated behaviors, and unwavering system oversight that builds a truly resilient defense.
Our commitment to patient safety drives us to remain vigilant, adapt our strategies, and continuously improve how we manage all potential sources of infection, including these critical points in our patient care environment. Protecting our patients requires us to see the unseen and to proactively manage the risks that hide in plain sight. We encourage you to share this guide with your teams and start a conversation about how your facility can enhance its own water safety protocols.

